















The last time I wrote about cancer it was for the Scientific American regarding how bacteria can be used as treatments so really it wasn’t even cancer I was talking about but when I was told about this doosey of a cancer I couldn’t help but write about it. This is significant for me as I am a bacteriologist who has spent a long time trying to avoid cancer (developing or writing about it), too many signalling pathways (imagine trying to memorise dozens of images like this), ick.
{kind=link}
Pseudomyxoma peritonei is a relatively rare cancer that literally is translated to mean “false mucinous tumor of the peritoneum”. The tumour is unusual because it’s of a very specific cell type resulting in an overproduction and accumulation of mucous in the abdominal cavity, also known as the peritoneum.
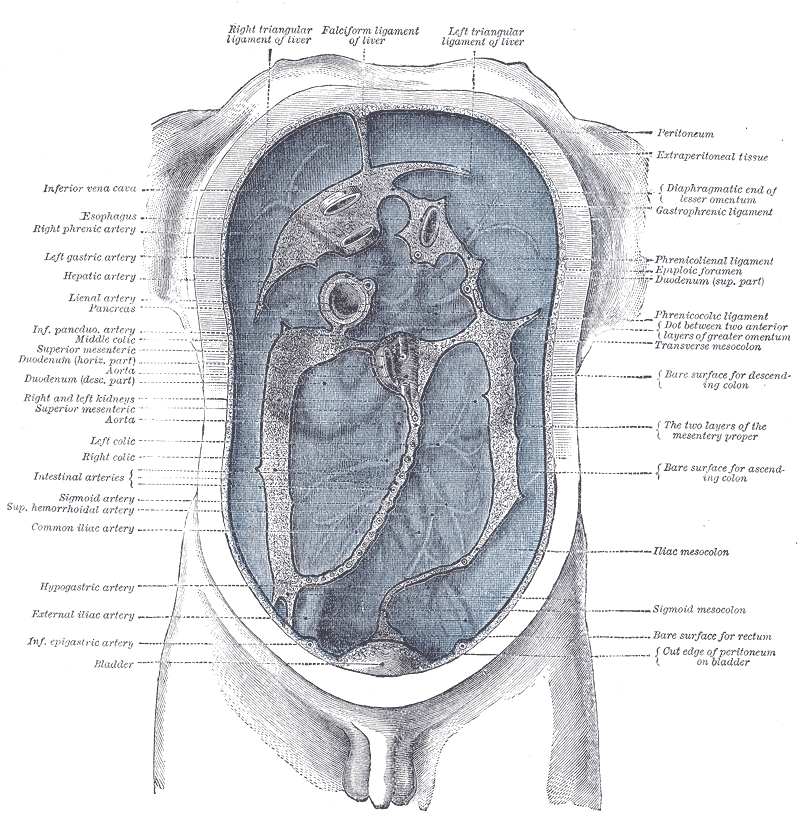 |
| I love using old Gray's Anatomy pictures. Click to embiggen but essentially the peritoneum is the blue bit. |
Although controversial it is currently believed that these cancers start in the appendix and over time the small internal cavity fills with proliferating tumour cells and they mucous they are producing until the organ becomes occluded. Once occluded the appendix will fill up like a fleshy mucous balloon (‘distends’ in medical speak) and eventually will explode (again, ‘rupture’ for the medicos out there) leaking the appendix’s contents into the abdominal cavity. But the tumour isn’t dead so the production of mucous continues slowly leaking more and more mucous.
I say the origin is ‘controversial’ because it is very hard to work out for this type of cancer. Ordinarily when you are diagnosed with cancer the doctor finds the biggest tumour, points to the middle of it and says it started right here. With disseminated cancers like those in Pseudomyxoma peritonei there is no tumour (hence the false part of its name) and you only realise you have it when your insides start to fill up with mucous.
Treating these cancers, as you can imagine is quite difficult. First you have to detect it. As the tumour is slow growing, and doesn’t form a solid tumour it is very hard to detect pathology early enough to prevent rupturing of the appendix and release of muck into the abdominal cavity. However, early detection allows for the removal of the appendix and with a bit of luck all the cancerous tissue with it.
If you don’t find it early consider yourself booked in for cytoreductive surgery also known as debulking. This kind of surgery involves opening you up and removing as much mucous as possible from the peritoneal cavity and removing organs that have been exposed to the mucous + cancerous cell mix. Generally this means patients will have the organs at the bottom of the abdomen removed including ovaries, uterus, bladder, parts of the small intestine, appendix, and parts of the liver.
Then you hope and wish that works.
 |
| That dotted line across the middle is referring to the "transpyloric plane", essentially everything under it is removed in during cytoreductive surgery. |
Alongside cytoreductive surgery you normally have your peritoneal cavity filled with good old chemotherapeutics.
Even if you survive all that it is very difficult to determine if the cancer is all gone for the same reasons it was hard to detect to begin with so patients look forward to a life of hospital waiting rooms as the current practice is to perform tests every 3 months to monitor for changes.
Commonly all of these techniques are now rolled into one operation called a Sugarbaker procedure. This procedure starts with complete cytoreductive tumour removal followed by surgical chemotherapeutic administration and removal of the right hemicolon, spleen, gallbladder, greater omentum and lesser omentum, uterus and ovaries in women and rectum in some cases then further work strips the peritoneum from the pelvis and diaphragm before removal of the tumour from the surface of the liver. Yeah, this operation takes about 10 hours and at the end you’re empty. That must be such a weird feeling.
Until my wife told me about this disease I had no idea such a cancer existed. Slow growing rare cancers rarely make it to public knowledge but they are really important. Pseudomyxoma peritonei does not kill many people per year as it is so rare but even after treatment the long term survival rates are only 40% or so, if you get it your in trouble.
Of all the cancers I’d like to never have (all of them) this one comes somewhere near the top of the list. As well as being deadly and impossible to treat with any confidence there’s a bunch of mucous and it’s the image of a burst appendix leaking dribbling mucous that I can’t shake.
Luckily, treatments are improving and survival rates are defiantly on the increase. One French study found that using specialised and expert services mortality falls to approximately 4% when malignancies do not develop and many sufferers are finding that successful surgery allows them to return to a close to normal life in most cases.
It’s always nice to find some good news after all the bad!
If you’re interested in finding out more info I would strongly suggest looking here for lay and in depth information and a support network for those diagnosed with this horrendous disease.
SHARE THIS!!!










References
- The Doctor's Doctor
- Surgical Oncology
- Hinson FL, & Ambrose NS (1998). Pseudomyxoma peritonei. The British journal of surgery, 85 (10), 1332-9 PMID: 9782010
- Sherer DM, Abulafia O, & Eliakim R (2001). Pseudomyxoma peritonei: a review of current literature. Gynecologic and obstetric investigation, 51 (2), 73-80 PMID: 11223697
- Brueggen C, Baird G, & Meisheid A (2007). Pseudomyxoma peritonei syndrome of appendiceal origin: an overview. Clinical journal of oncology nursing, 11 (4), 525-32 PMID: 17723965
- Glehen O, Gilly FN, Boutitie F, Bereder JM, Quenet F, Sideris L, Mansvelt B, Lorimier G, Msika S, & Elias D (2010). Toward curative treatment of peritoneal carcinomatosis from nonovarian origin by cytoreductive surgery combined with perioperative intraperitoneal chemotherapy: A multi-institutional study of 1290 patients. Cancer, 116 (24), 5608-18 PMID: 20737573
hey James, interesting article. I had the surgery and HIPEC treatment for this, appendix cancer, last January. I wrote about it on my blog, www.oncoloblogy.com.
ReplyDeleteDan
Hey Dan,
ReplyDeleteI just checked out your blog. Its very cool. I'm sorry to hear about your surgery but I hope things are looking better for you.
If you think others might like it feel free to share it with them, I just hope I covered the info well enough.
Thanks for checking out the blog :)
James, good article. I was diagnosed with Pseudomyxoma Peritonei in 2010 and had cytoreductive suregery and HIPEC (hyperthermic intraperitoneal chemotherapy) followed by 4 days of EPIC (early postoperative intraperitoneal chemotherapy) 9 months ago.
ReplyDeleteIt is such a rare disease and it is so much easier if you can find other people who understand what you are going through. I came across a fantastic group on Facebook and a registered charity which have helped me a lot. There is a link to the Fb group on the website:
Pseudomyxoma Survivor